Blunt abdominal trauma is encountered in day-to-day life in the adult and pediatric age group populations. Most are caused by road traffic accidents, falls from a bicycle, blunt trauma from football to the abdomen, injury to the abdomen from edges of table/desk, etc. A blunt trauma to the abdomen causes injury primarily to solid organs - liver, spleen, pancreas, mesenteric tear, and diaphragm rupture. Hollow viscus like intestines and stomachs get spared commonly. Blunt abdominal trauma cases should not be overlooked and urgent medical attention and evaluation are musts. Diaphragmatic rupture is a rare condition after blunt abdominal trauma and can be easily misdiagnosed through a lack of proper evaluation. The mechanism behind this is sudden increased trans-abdominal pressure which causes rupture of the diaphragm and migration of abdominal organs like the stomach, spleen, and colon into the thoracic cavity.
Here we present a case of chronic Diaphragmatic hernias where the patient a 20-year-old female was referred to our hospital with complaints of breathing difficulty, food regurgitation, and recurrent vomiting episodes along with abdominal fullness and chest pain for the last few years. The patient had a history of blunt abdominal trauma while playing football a few years back, following which she took treatment at some outside hospital but remained misdiagnosed of her condition. A detailed radiological investigation and CT scan showed left-side Diaphragmatic Rupture with herniation of the stomach and bowel inside the left Hemi thorax with collapsed left lung.
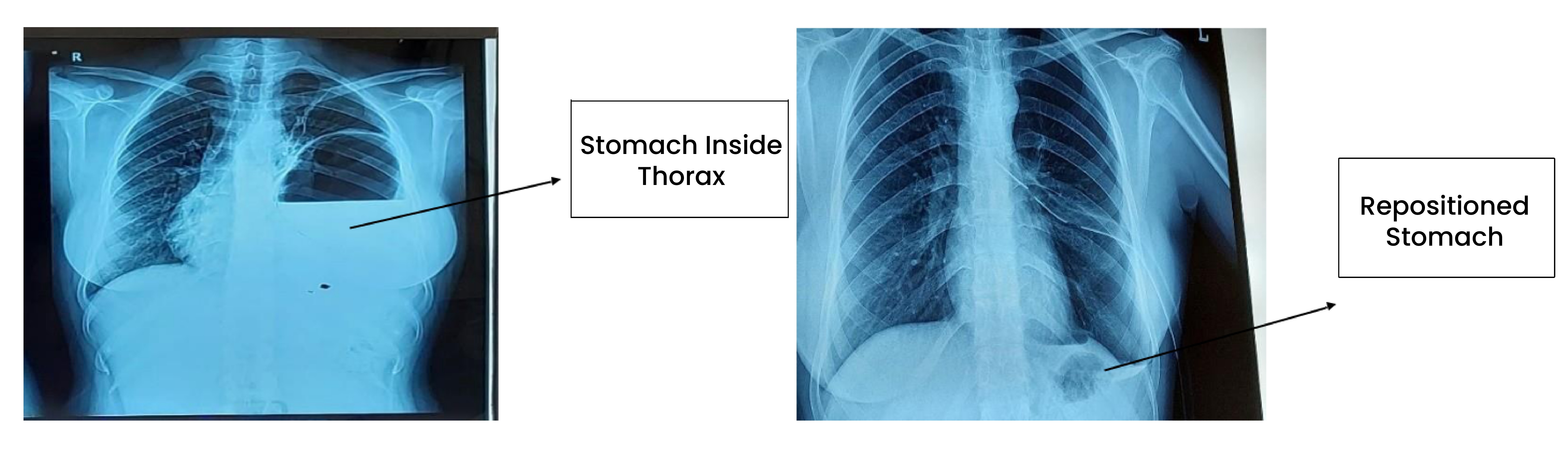
The stomach inside Thorax Repositioned Stomach
(X-Ray before surgery) (X-Ray after surgery)
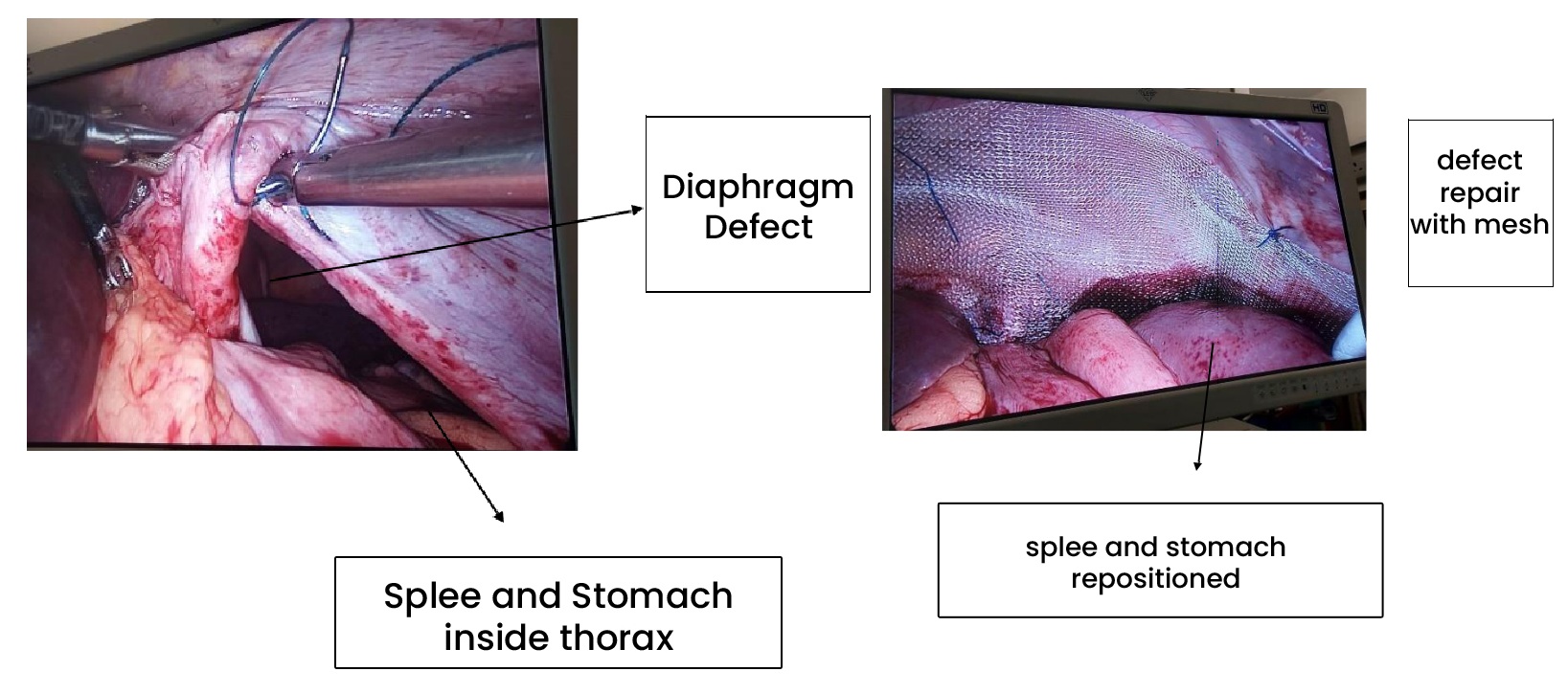
After evaluation patient and attendants counseled them on her condition and planned for the Laparoscopic Diaphragmatic repair. Intraoperatively we found not only the stomach but part of her large intestine and the whole of her spleen were displaced into the left Hemi thorax of the patient. Managing this patient via laparoscopic approach was a difficult task, but after the removal of dense adhesion, we were able to reduce all the contents back into the abdomen from the thorax and repaired the large diaphragmatic defect in layers with the placement of mesh along with Intercoastal drainage tube insertion in left Hemi thorax.
The patient was discharged on postoperative day 4 in stable condition, the follow-up period was uneventful and now the patient is doing well free from all comorbidities related to her condition.
Take home message is never ever ignore abdominal injuries as they may manifest into some serious life-threatening events and require surgical intervention.